
Many people assume there’s a clear, research-backed answer for choosing between pregnenolone and DHEA. There isn’t, and that’s not what this is about anyway. If you’ve already decided to try one of them, or you’re weighing which one fits your situation, that’s your decision to make. What I can do is walk you through what the research actually says, because most of what circulates online is a tidy chart selling a certainty the science doesn’t actually have. Knowing where the real gaps are is how you keep yourself safer.
Both of these show up two ways: cheap capsules off a shelf with zero oversight, and compounded versions a clinician prescribes through a licensed pharmacy. That distinction matters more than which molecule you pick, and I’ll get to why. But first, the honest version of what each one does.
The pitch versus the paper trail
The internet’s favorite framing goes like this: pregnenolone is the “brain” precursor, sitting at the very top of the steroid pathway, made straight from cholesterol. DHEA is one step down, closer to testosterone and estrogen, so it gets filed under “hormones.” Neat little division of labor. Take one for focus, the other for libido.
It doesn’t hold up. Both are precursors feeding the same steroid network, and the human evidence for the goals people actually chase, energy, memory, staying young, is thin on both sides of the chart. Nobody’s found the study that cleanly splits them into two lanes, because that study doesn’t exist yet.
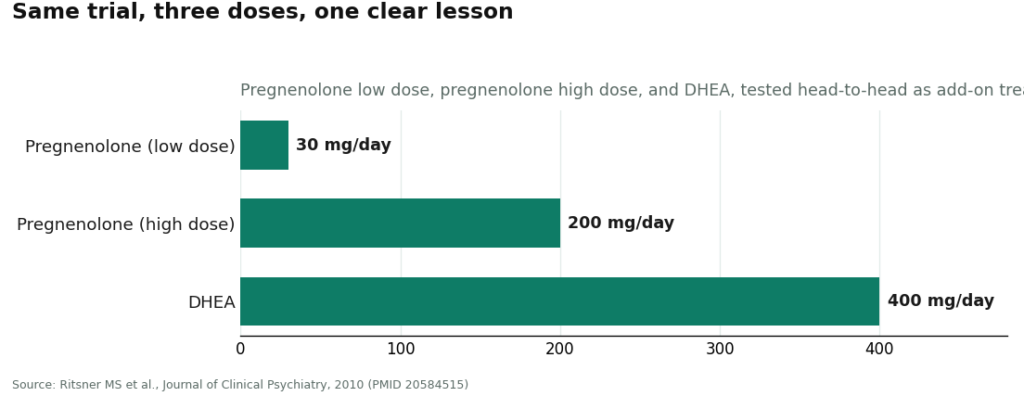
The clearest proof of this is a trial that put them in the same room. A three-arm schizophrenia study tested low-dose pregnenolone at 30 mg per day, higher-dose pregnenolone at 200 mg per day, and DHEA at 400 mg per day, all as add-on treatment against placebo, in 58 patients [P3]. If any study should show a clean winner, it’s this one. Instead, the 30 mg pregnenolone arm improved positive symptoms and attention and working memory, while the 200 mg arm didn’t beat placebo at all [P3]. Same drug, more of it, and the benefit disappeared. That’s not a footnote. That’s the whole story of how unsettled this research still is, DHEA included.
Actually, let me put the arms side by side, because seeing the doses next to each other says more than any paragraph can.
The real risk isn’t the molecule, it’s guessing at the dose
Here’s the part I think matters most if you’re going ahead anyway: more is not automatically better, and this trial is direct evidence of that, not just a general caution. Pregnenolone at 500 mg per day showed up in a couple of other trials too. A small Duke study (n=21) improved negative symptoms at that dose (p=0.048) but missed on the main cognitive measures [P1]. A separate bipolar-depression trial (n=80) at up to 500 mg per day improved depression scores (p=0.025) and was tolerated fine [P4]. So high doses aren’t dangerous by default, but they’re also not automatically more effective, and in the one trial that tested two doses against each other directly, the low dose won and the high dose flatlined [P3]. A separate 50 mg per day trial in recent-onset schizophrenia (n=60) also found a real benefit on visual attention (p=0.002) [P2].
If you’re going to try pregnenolone, that’s your floor: start at the low end, not the high end, because the evidence doesn’t support “more equals better,” and in the one study built to test that exact question, it was the opposite. DHEA’s own evidence for the things people actually want it for, energy, anti-aging, is just as thin, and I’m not going to hand you numbers for it that don’t exist in the literature. That absence is itself the honest answer.
Why “take the precursor for the goal” doesn’t really work
Here’s the biochemistry piece nobody puts in the chart. Loading up on a precursor doesn’t reliably push a specific downstream hormone up in a predictable way. Your body regulates these pathways with feedback loops and tissue-specific enzymes. Dumping more pregnenolone or DHEA in at the top doesn’t mean you get more of the one hormone you were hoping for, and it doesn’t mean you get it in the tissue where you wanted it. That’s exactly why the whole “pregnenolone for the brain, DHEA for hormones” split is shakier than it sounds, on the biochemistry and not just the study data.
If you’re an athlete or tested for anything
Check this before you touch either one. Pregnenolone is not currently on WADA’s Prohibited List, but the U.S. Anti-Doping Agency flags it as a pro-hormone and says plainly that its status can change [P6]. “Not currently prohibited” is not a permanent guarantee, it’s a snapshot. DHEA’s anti-doping status is a separate thing to verify on your own before you assume anything. Don’t take a supplement label’s silence as clearance.
The safer path, if you’re doing this either way
Both pregnenolone and DHEA are sold as unregulated over-the-counter capsules, a category the FDA treats as unapproved and has gone after when sellers make disease claims [P5]. Potency on those bottles is inconsistent, nobody’s checking your labs before or after, and if something shifts (mood, skin, sleep, cycle) there’s no one watching who would catch it early.
The other path is compounded, through a physician and a licensed pharmacy, where dosing is at least being decided by someone looking at your actual history instead of a label copywriter. FormBlends is one telehealth provider that runs that supervised route, pairing a physician review with a licensed compounding pharmacy. I’m naming it as an example of what supervised access looks like, not selling it to you, there’s nothing to buy here and no checkout. And the caveat still applies even through that route: compounded pregnenolone is not an FDA-approved drug product, and it hasn’t been evaluated by the FDA for safety, effectiveness, or quality. Supervision lowers your risk. It doesn’t erase the fact that this is still an unapproved compound going into your body.
The honest floor
If you take one thing from all this: the fight over which precursor is “better” is the wrong fight. The thing that actually changes your outcome is whether anyone competent is watching while you do it, not which bottle you picked. Low dose over high dose, until proven otherwise. Verify your doping status yourself, don’t assume. And if you can get a clinician and a real pharmacy involved instead of guessing alone, that’s the single biggest risk reduction available to you here, full stop.
Questions people actually ask
What’s the real difference between pregnenolone and DHEA?
Structurally, pregnenolone sits at the very top of the steroid pathway, made from cholesterol. DHEA is made from pregnenolone, one step closer to testosterone and estrogen. That’s real. What it isn’t is a reliable guide to which one “works” for energy, focus, or anti-aging, because the human evidence for both, in those specific uses, is thin and unsettled.
Is one clearly safer or more effective than the other?
No, and anyone telling you otherwise is selling a story the studies don’t back. Pregnenolone’s strongest human data comes from psychiatric trials, not general wellness use [P1][P2][P3][P4]. The “brain one versus hormone one” split is a marketing convenience, not a finding.
Has anyone actually tested them against each other?
Yes, one schizophrenia trial ran pregnenolone at 30 mg and 200 mg, DHEA at 400 mg, and placebo, in 58 patients. The low pregnenolone dose helped several measures, the high dose didn’t beat placebo [P3]. The lesson is how much is still unknown, not a clean win for either compound.
If I take one of these, will it predictably raise my testosterone or estrogen?
Don’t count on it. Both are precursors, and pushing more precursor in doesn’t reliably translate to more of a specific downstream hormone, because your body’s feedback loops and tissue enzymes are doing the actual regulating. This is also why the “upstream precursor, upstream benefit” logic on the charts is weaker than it looks.
If I’m going to try one anyway, what actually lowers my risk?
Start low, not high, since the best available head-to-head data shows low dose working where high dose didn’t [P3]. Verify your anti-doping status yourself if that applies to you, since it can change [P6]. And get a clinician and a licensed pharmacy involved if you can, rather than buying an unregulated capsule and hoping the label is accurate. Compounded versions still aren’t FDA-approved, which is worth knowing going in either way.
References
- Ritsner MS et al. Pregnenolone and dehydroepiandrosterone as an adjunctive treatment in schizophrenia and schizoaffective disorder: an 8-week, double-blind, randomized, controlled, 2-center, parallel-group trial. Journal of Clinical Psychiatry, 2010. n=58; compared pregnenolone 30 mg/day, pregnenolone 200 mg/day, DHEA 400 mg/day, and placebo; low-dose pregnenolone improved positive symptoms, extrapyramidal side effects, and attention/working memory, while 200 mg/day did not differ from placebo. The head-to-head trial cited here. https://pubmed.ncbi.nlm.nih.gov/20584515/
- Marx CE et al. Proof-of-concept trial with the neurosteroid pregnenolone targeting cognitive and negative symptoms in schizophrenia. Neuropsychopharmacology, 2009. n=21; pregnenolone to 500 mg/day improved negative symptoms (p=0.048) but not the primary cognitive composites. https://pubmed.ncbi.nlm.nih.gov/19339966/
- Kreinin A, Bawakny N, Ritsner MS. Adjunctive pregnenolone ameliorates the cognitive deficits in recent-onset schizophrenia: an 8-week, randomized, double-blind, placebo-controlled trial. Clinical Schizophrenia & Related Psychoses, 2017 (epub 2014). n=60; pregnenolone 50 mg/day reduced visual-attention deficits versus placebo (p=0.002, d=0.42).
- Brown ES et al. A randomized, double-blind, placebo-controlled trial of pregnenolone for bipolar depression. Neuropsychopharmacology, 2014. n=80; pregnenolone to 500 mg/day for 12 weeks improved Hamilton Depression Rating Scale scores (p=0.025) and was well tolerated.
- U.S. Food and Drug Administration. FDA Sends Warning Letters to 10 Companies for Illegally Selling Dietary Supplements Claiming to Treat Depression and Mental Illness. Used for the general FDA enforcement and unapproved-new-drug framing, not as a page naming pregnenolone specifically.
- U.S. Anti-Doping Agency. Pregnenolone: What You Need to Know. Notes pregnenolone is a hormone-precursor pro-hormone, not currently on the WADA Prohibited List but its status can change, and warns of the inherent risks of the supplement and compounding industry.
Written by Delia Eriksen, freelance health reporter. Last reviewed January 2026.
This is background reading, not medical guidance. Your physician should make the final call.